


These days, Dale Cunningham is taking extra time to appreciate the sights and sounds of spring in New England.
On a recent walk through a park nearby, Cunningham soaked up the sun and stopped to appreciate a passing songbird.
“It's so good that spring is finally here,” Cunningham said. “I'm just glad to be alive right now.”
She has all the more reason to be joyful.
In January, Cunningham, 69, showed up at the emergency room for what her doctor thought was a potentially critical gallbladder condition.
“The waiting room was very full of patients sitting on the window sills, people were vomiting in the trash cans,” she said. “If I didn't know someone there, lord knows how long I would have waited.”
Cunningham said she was admitted into the ER after making a few calls — she works at the hospital, Yale-owned Lawrence + Memorial in New London, as a neonatal nurse.
At the ER she learned she would need to be hospitalized, but an inpatient room was not available.
“I stayed there [in the ER] for two days, almost,” she said. “There was 40 people waiting for beds.”
Later, doctors would tell her that she had stage 2 bile duct cancer – part of her liver had atrophied and died.
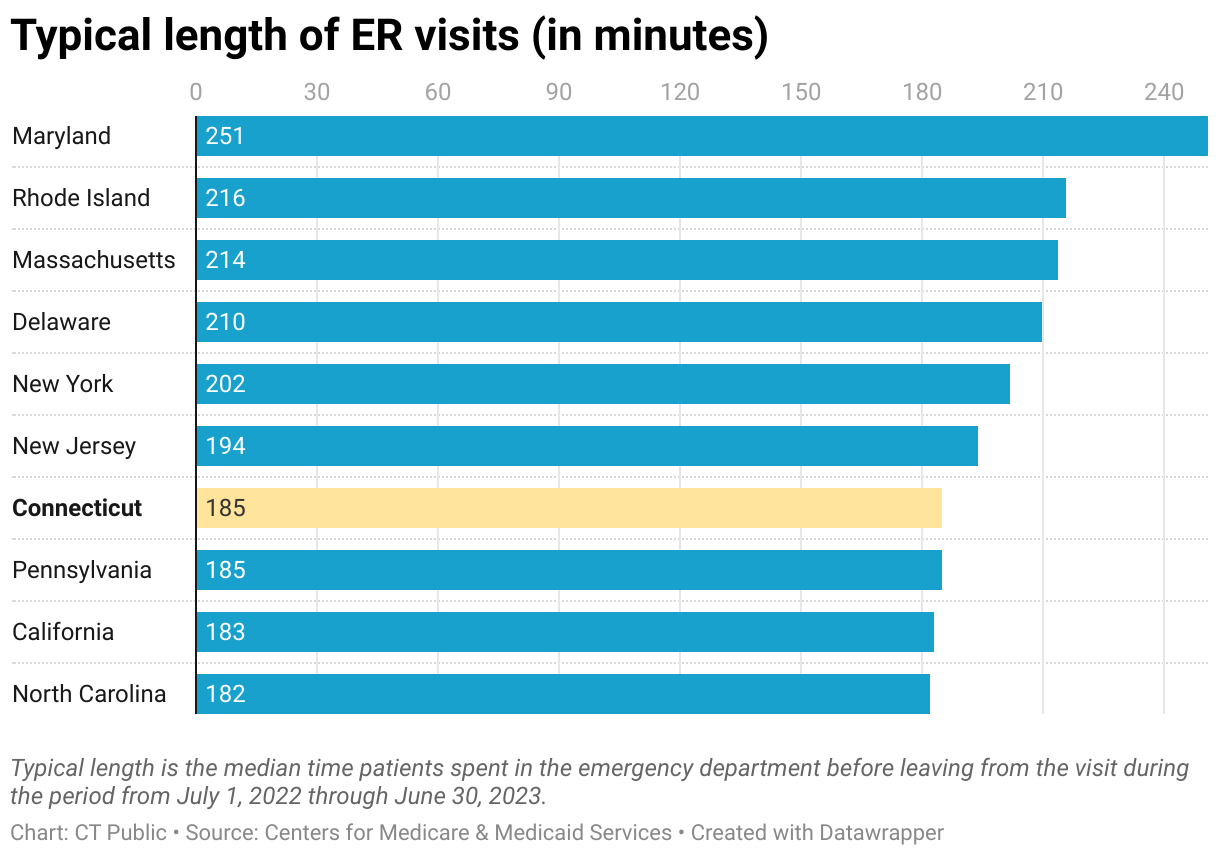
Cunningham’s experience waiting for care in the emergency department is not unique. In ERs across Connecticut, patients are facing increasingly long wait times. Federal data shows a typical ER visit now lasts more than three hours.
Connecticut is tied for seventh place in the entire country for longest emergency room visits.
The reasons are multifold.
Lawrence + Memorial said in a statement that ER overcrowding has worsened since the COVID-19 pandemic — the acute shortage in skilled nursing, home care, and rehab, is delaying moving patients out of the hospital.
Connecticut Children’s ER sees around 60,000 patients a year with more children presenting with more complex issues that have to be evaluated in the emergency department, said Dr. John Brancato, division head of emergency medicine at the hospital.
“So they are there for a longer period of time,” he said. “And then there's a well known increase in patients with behavioral health concerns.”
Brancato is member of a state committee — The Emergency Department Boarding and Crowding Working Group — advising lawmakers to step in and address what they say is a public health crisis.
At the state Capitol in April, two of Brancato’s colleagues on the committee — ER doctors Christopher Moore, professor of emergency medicine at Yale, and Gregory Shangold, president of the Connecticut State Medical Society — met with state Sen. Saud Anwar, chair of the Public Health Committee, to help shepherd S.B. 181 through the House.
The bill requires hospitals to start reporting information next year about back-ups in the emergency department, including the number of patients in the ER, the number waiting to get into the ER, the number waiting for a hospital bed to open up, and total wait times.
“We see 50%, 60%, 70% of the emergency department is occupied by patients waiting for beds up in the hospital,” Shangold said.
The bill won unanimous approval in the Senate, and passed in the House with 140 of the 149 voting members in favor.
Moore said much like the proverbial frog boiling slowly in a pot of water, it has become normalized to take care of patients, even sick, elderly patients with gastrointestinal bleeding, in the hallways. “That really shouldn't be the norm, but we've gotten used to it gradually over time,” he said.
In an interim report published earlier this year, the workgroup pointed to emergency room boarding as the primary driver behind increasing wait times. Boarding occurs when staff decide to admit a patient to the hospital, but the facility doesn’t have enough capacity to provide an inpatient bed, leaving the patient waiting in the ER. Some of the factors that drive boarding are insufficient staffing, delays in cleaning available beds, and delays transferring patients to other facilities.
“Connecticut has the opportunity to put a lens on it, to understand that it is a patient care issue, which is why we are asking people to look at the data and to frame it as a quality measure,” Moore said.
The Connecticut Hospital Association was in favor of the amended bill and said it appreciates the support of the legislature.
Finding solutions is important because backups in the emergency room can cause serious harm to patients. Studies show ER crowding increases exposure to medical errors, like administering the wrong medication. It also slows down treatment of serious conditions like heart attacks and strokes.
“If somebody is going to have an emergency and they go to the emergency room and nobody can see you, there’s no room to be seen or there’s no place to be in the emergency room, your outcome is going to be poor,” Anwar said.
Patient testimonials in support of the bill paint a dire picture.
Christine Macaluso said she went to the Yale ER on Goose Lane with what she thought was appendicitis on Nov. 8, 2023.
Macaluso needed to be transferred to the Yale campus on York Street for further testing, but was held at Goose Lane for almost 20 hours while waiting for a bed to open and for the transport service, she wrote.
“While the staff at Goose Lane was attentive, they only had the resources to control my pain, not to do the necessary testing that eventually led to a cancer diagnosis. The ER did not have food or other medications I needed [for preexisting conditions] available,” she said. “A 20 hour wait in the ER, when in pain with no idea why, is too long.”
Nancy Sylvain wrote in her testimony that she stayed for 52 hours in a hallway in the ER of Yale New Haven Hospital. “I was in extreme pain, unable to sit, stand, or lay down for more than a few minutes at a time,” she said. “After finally getting a bed, I exhibited stroke symptoms and was whisked away by the stroke team.”
It turned out that Sylvain did not have a stroke, but she had meningitis in her brain and spinal cord with Bell’s Palsy as a result of undiagnosed Lyme disease.
“My experience was unfortunately not uncommon, as the emergency room was packed with other patients also waiting for a bed,” she wrote. “I was shocked to see that patients like myself also lined many hallways, as the emergency room was too full to accommodate them.”

Michael Holmes, chief operating officer at Yale New Haven Hospital, said part of the challenge is that hospitals serve as a safety net for the community, and never turn away patients.
“Other parts of the health care delivery close at five o'clock. They're not open on weekends,” Holmes said. “Your local emergency department and their team are here 24/7, 365.”
And because of that load, patients and families continue to struggle.
In the case of Dr. Sue Sundaresan’s 87-year-old father-in-law, the family said ER doctors at Hartford Hospital were too stretched to attend to a non life-threatening situation.
“Every time he swallowed, every time he ate, his nose would start bleeding,” she said.
Sundaresan tried to get a nurse to stop the bleeding and spoke to other ER staff, but she said no one came. “So now it's pouring down his face. We have nothing to mop it with,” she said. “I literally had to go outside and find towels to actually close this up.”
“I don't know if there was a shortage of staffing, or it was just a lack of empathy to have an 87-year-old man sitting there who had not eaten since the previous night,” she said. “No one was coming to check on him because even though he was [in the ER], I think it was not a life threatening emergency."
Sundaresan’s father-in-law was first seen at an urgent care for the nosebleed, where he was diagnosed with atrial fibrillation and transported by ambulance to Hartford Hospital.
She said when he was taken to an in-patient room after waiting for close to nine hours in the ER, an ENT specialist told her that he should have been seen sooner for the nose bleed.
A medical doctor herself, Sundaresan said she knew that her father-in-law would not be able to get sedated for the procedure he needed to undergo to reverse the sudden abnormal heart rhythm.
Hartford Hospital said the organization is committed to identifying solutions to ER overcrowding, including filing requests to add more bed capacity in some locations.
A spokesperson said recent openings that include 29 urgent care centers, five pharmacy clinics and three virtual health stations located in places like grocery stores.
“All of these offer improved access to patients who need non life-threatening medical care,” the spokesperson said.
Lining up financial incentives
Physicians say there are differences between institutions in terms of the reasons why some hospitals board more than others.
One common denominator is incentives.
“If someone is admitted to the hospital, the hospital’s going to get the same amount whether they have their whole stay in a hallway in the emergency department or they have a private in-patient bed,” Moore said. “I’m not saying that the hospitals don’t want to get them to an in-patient bed but it’s not necessarily financially beneficial to do so.”
The other possibility is the scheduling of surgeries. “For example, if the hospitals wanted to institute surgical smoothing – scheduling of elective surgical procedures on nights and weekends – that would be a way to address the issue,” he said.
Moore’s observations mirror those of several ER physicians across the country.
But the Connecticut Hospital Association strongly disagreed that decisions about ER patient admissions or inpatient bed availability are made based on financial incentives, and that providing surgeries to patients causes ER boarding.
In a January survey by the state committee on ER boarding in Connecticut, ER doctors said the Medicare three day rule was exacerbating the crisis. Under the rule, people insured by Medicare must spend three days in the hospital as in-patients before they’re eligible for coverage for treatment in a skilled nursing facility. When in-patient beds aren’t available, people spend those days in the emergency room. This rule was relaxed during the peak of the COVID-19 pandemic, but has since been reinstituted.
Solutions underway statewide
One solution is expanding hospital capacity. Connecticut Children’s is opening an eight-story unit next year and the ER at Yale’s St Raphael's campus is adding 51 treatment spaces. And the new ER annex at Yale New Haven Hospital has 35 additional beds.
Lawrence + Memorial is encouraging patients to review ER wait times on the hospital website to determine if perhaps urgent care or walk-in centers might be more appropriate.
ER boarding is the result of longstanding health care problems — population health, increasing acuity of patients, primary care access, prior insurance authorization, and transportation to other medical facilities, Dr. Arjun Venkatesh, chief of emergency medicine at Yale, said.
“We need the rest of that outpatient system to be lifted and elevated so that there's access to care beyond that acute event that happens,” he said. “And that's true for overdose. It's true for a stroke. It's true for every other kind of condition you can think of.”
Yale created a post-discharge extended care clinic where patients discharged from the ER could go for follow-up care if they do not have a primary care physician. Yale has also partnered with its urgent care clinics to take patients initially stabilized in the ER for follow-on care, and established a dedicated psychiatric emergency unit.
“The challenge is that as we expand and as we create these alternative pathways to care, the rest of the broader system is shrinking,” Venkatesh said.
Lawmakers should have a better understanding of the circumstances by early next year. State hospitals are required to file reports on emergency room delays and potential solutions by March 2025.
Connecticut Public’s Michayla Savitt contributed to this story.
